LONG-TERM DISEASE CONTROL AND EXCELLENT QUALITY OF LIFE WITH FIRST-LINE RIBOCICLIB PLUS LETROZOLE TREATMENT IN A GERIATRIC PATIENT WITH METASTATIC BREAST CANCER
Patient: 77 years old, mother of three children and grandmother of four.
In the past she had bilateral breast silicone implants surgery for breast augmentation and she also underwent hysterectomy for leiomyomas but she didn’t have bilateral oophorosalpingectomy.
February 2018: Age 75, she was admitted in a private clinic for lower abdominal pain.
The CT scan of the abdomen revealed ascites in the abdomen and pelvis and diffuse peritoneal carcinomatosis.
The original diagnostic hypothesis was ovarian cancer.
Clinical breast examination:
Hard palpable mass in the periaureolar zone of the right breast with skin retraction and hardening of the external quadrants of the right breast and palpable bilateral axillary lymph nodes.
Blood test:
Without pathological findings.
Tumor markers:
CEA: 75.5 ng/ml, CA 15-3: 265.4 U/ml, CA 125: 158.7 U/ml.
CT scan of the abdomen:
Ascites in the abdomen and pelvis and diffuse peritoneal carcinomatosis.
Bilateral mammography, bilateral breast and axillary ultrasound:
Bilateral retroglandular silicon implants. Skin retraction in the inferior quadrant of the right breast with no observation of microcalcifications in the periaureolar external quadrant in an area of 2 cm of diameter, multiple hypoechogenic cysts in both breasts, multiple enlarged bilateral axillary lymph nodes, bigger in the right axilla with extension to levels I, II and III.
Breast MRI:
Multifocal infiltrating mass of the right breast causing deformation and retraction of the right breast with suspicious bilateral axillary lymph nodes. At the left breast, presence of multiple millimetric contrast enhancement, the biggest of all, in the external quadrant measures 4 mm.
Exploratory laparoscopy with multiple biopsies:
Diffuse peritoneal carcinomatosis with multiple intestinal and gastric implants, carcinomatosis of the parietal peritoneum mostly in the Douglas.
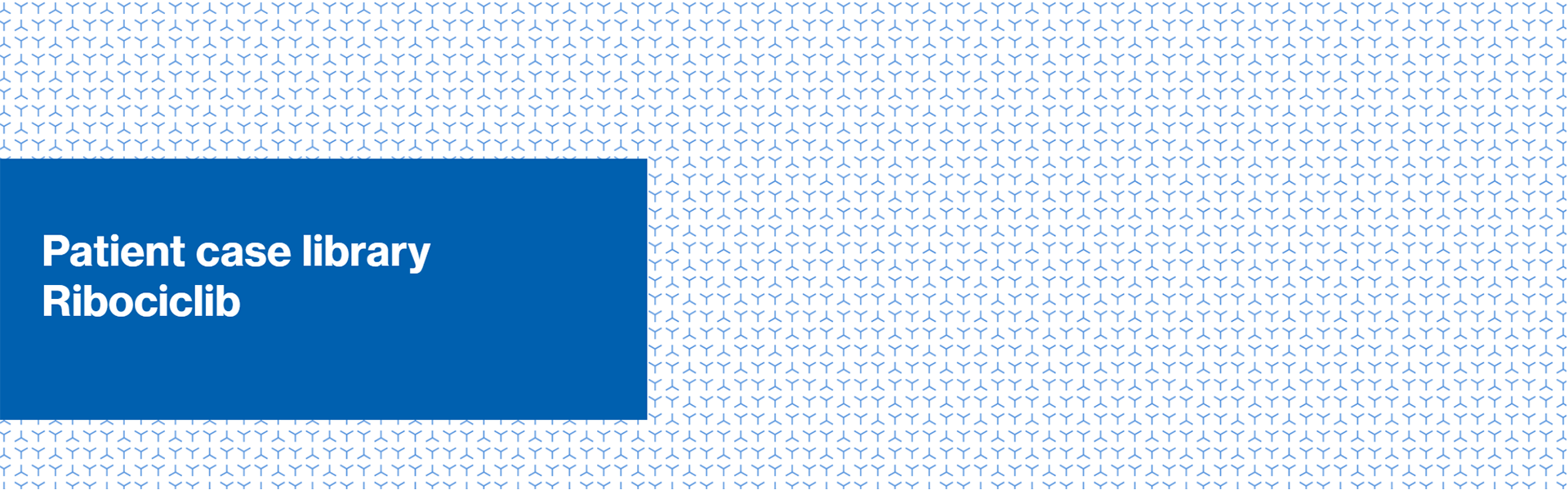
PET scan:
Diffuse peritoneal carcinomatosis mostly evident at the epigastrium, mesogastrium and at the left side of the abdomen, and presence of ascites in the Douglas. Diffuse contrast enhancement bilaterally in the breasts more evident at the right breast. Moderate FDG-active lymph nodes in both axillary regions mainly at the right (diameter 1 cm, SUV max 1.5). Several bone lesions of mixed type, slightly FDG-active, in multiple cervical, thoracic, lumbar vertebras and bones of the pelvis bilaterally. Collaterally, diffuse uptake of the tracer in the thyroid gland, in first hypothesis thyroiditis.
Multiple abdominal biopsies and immunohistochemical analysis of the right parietal
peritoneum:
Metastases of carcinoma compatible with lobular breast carcinoma, fragments of ovarian parenchima infiltrated by breast carcinoma, ER: 95%, PR: 95%, Ki-67: 10%, c-erbB-2 score: 0.
Biopsy and immunohistochemical analysis of the right breast:
Lobular invasive carcinoma ER: 100%, PR: 0%, Ki-67: 5%, c-erbB-2 score: 0.
ECOG (Eastern Cooperative Oncology Group performance status):
1.
Genetical testing:
Not done.
Diagnosis:
Primary metastatic bilateral lobular invasive carcinoma of the breasts, with metastases to bilateral axillary lymph nodes, diffuse peritoneal carcinomatosis, metastases to the right ovary, diffuse bone metastases (cervical, thoracic, lumbar vertebras and multiple bone metastases of the pelvis). The breast cancer is hormonal receptor positive and HER2-negative.
Treatment:
Letrozole 2.5mg/d + ribociclib 600mg/d (d1-d21, q28d), since March 2018.
Denosumab 120mg sc. q4 weeks, since August 2018 (patient enrolled in the SAKK 96/12 study, arm A:
denosumab monthly).
Additional medications:
Calcium + vitamin D3.
Duration of treatment:
Until progression of disease or unacceptable toxicity.
Patient monitoring strategy:
Complete blood count and liver function values every 2 weeks for the first two cycles, then every 4 weeks.
Tumour markers at the beginning of every cycle.
ECG every 2 weeks within the first cycle of ribociclib and at the beginning of the second cycle.
Tumour assessment strategy:
CT scan or PET-CT every 12 weeks.
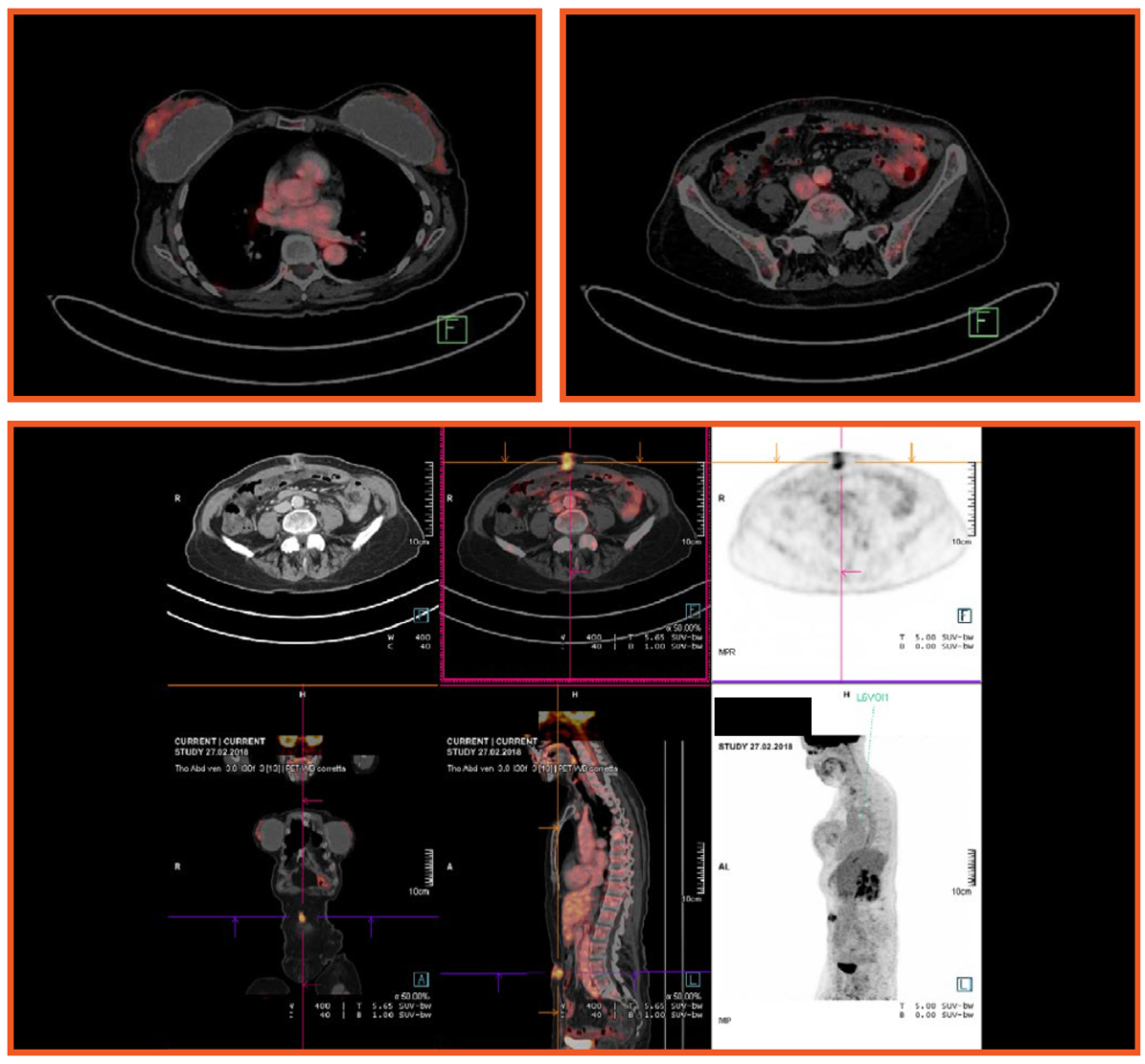
Monitoring:
PET-CT (last 27.09.2019): metabolic resolution of the disease in the peritoneum and lymph nodes and of skeletal lesions, low and diffuse dishomogeneous positivity in both breasts, partial remission of disease (PR), according to RECIST criteria.
Tumour markers:
CEA: 6.8 ng/ml, CA 15-3: 19.6 U/ml, CA 125: 6.2 U/ml (21.10.2019).
Adverse events:
Fatigue G1, leucocytopenia, neutropenia (max. G3), hot flashes.
Quality of life:
Good.
ECOG:
PS 0.
Impact on hobbies, activities:
Every day performs 1 hour walk and climbs on 400 steps in excellent conditions. During summer she went regularly for swimming in the lake. In September 2019 she visited Armenia on vacation for 1 week to celebrate the wedding of her son.
Patient feedback:
Very positive, enthusiastic.


After 2 cycles of treatment, from May 2018 the abdominal pain disappeared. The patient is now on letrozole/ribociclib for 20 months. At the first re-evaluation of disease after 3 months at the PET/CT there was not any ascites in the abdomen.
She has a really good quality of life, maintains her activities and hobbies and has always a positive attitude.
FEMALE, 65-YEAR-OLD
| Patient presentation and diagnosis 2018 |
March |
September 2019 |
| DIAGNOSIS: Metastatic bilateral breast lobular invasive carcinoma, axillary lymph nodes, diffuse peritoneal carcinomatosis, right ovarian and bone metastases Hormonal receptor positive, HER2- |
Partial remission of disease PET/CT: metabolic resolution of the disease in the peritoneum, lymph nodes, sceletal lesions, low and diffuse dishomogeneous positivity in both breasts Fatigue G1, leucocytopenia, neutropenia (max. G3), hot flashes Good QoL ECOG 0 |
|
| TREATMENT: ribociclib 600mg for 21 days + letrozole 2.5mg once daily denosumab 120mg 4-weekly (from August 2018) |
Treatment ongoing |
In this case the combination of ribociclib with the aromatase inhibitor letrozole have provided a long-lasting disease control, with very few and acceptable adverse events and an excellent quality of life.
- Kisqali. SUMMARY OF PRODUCT CHARACTERISTICS. August 2017
- Hortobagyi GN et al. Updated results from MONALEESA-2, a phase III trial of first-line Kisqali plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018 Jul 1;29(7):1541-1547
Swiss medcal network, Clinica Sant’Anna, Centre for Senology, Lugano, Switzerland
This case was created by Michail Kouros, MD
Author takes full responsibility for presented information which reflect author’s stand/practice and might not be in line with local approved SmPC.