IMPORTANCE OF PROMPT RECOGNITION OF INFECTIONS DURING TREATMENT WITH RIBOCICLIB TO PREVENT SERIOUS INFECTIOUS COMPLICATIONS
The patient had left modified radical mastectomy at the age of 51 due to breast cancer:
- invasive ductal carcinoma, 4,5 cm large, grade III, ER 100%, PR 95%, MIB-1 20%, HER2 status negative,
- 7/28 lymph nodes positive,
- genetic testing negative, PIK3CA mutation not found in the primary tumor,
- adjuvant treatment: chemotherapy with anthracyclines and taxanes, radiation therapy and tamoxifen.
She relapsed after 16 months of adjuvant tamoxifen treatment with bone metastases and was treated in 1st line with ribociclib and letrozole:
- She remained progression free for almost 4 years
- She suffered one serious adverse event: erysipelas with sepsis due to delayed consultation of the doctor after the injury to her finger during gardening.
She is now on her 3rd line of treatment, fully active with good quality of life.
Female, born in 1965
Family history:
- Breast cancer: mother (at 69 years) and maternal relatives: aunt (at 50 years), grandmother (as elderly) → genetic testing negative
Comorbidities:
- levothyroxine 50 μg/day due to hypothyroidism after treatment with radioiodine
3/2016: left modified radical mastectomy due to palpable breast cancer was done:
- invasive ductal carcinoma, 4,5 cm large, grade III, ER 100%, PR 95%, MIB-1 20%, HER2 status negative
- 7/28 lymph nodes positive
Adjuvant treatment:
- Chemotherapy: anthracyclines followed by taxanes,
- 9/2016: start of adjuvant tamoxifen + adjuvant radiotherapy → follow up visits NAD till 12/2017: elevated CA15-3 (274 kU/l)
|
Clinical information |
|
|
Age |
52 years |
|
Menopausal status |
postmenopausal |
|
Visceral disease |
None |
|
Adjuvant endocrine treatment duration (Subcategories: prior/on/after adjuvant) |
On tamoxifen |
|
Metastasis localization and numbers |
Bones (two: in pelvis and 5th thoracic vertebra) |
|
Medication |
Letrozole + ribociclib |
|
Geriatric assessment (if available) |
/ |
|
Comorbidities and concomitant treatment |
Hypothyrosis (levothyroxine 50 μgm/day) |
|
Previous treatments |
tamoxifen |
|
Genetic test results (if available) |
negative |
|
Personal information |
|
|
Lifestyle (Subcategories: Activities, hobbies, habits, smoking, eating habits, obesity, exercise) |
Non smoker, regular exercise |
|
Patient treatment preferences (Subcategories: Cancer treatment: IV, Oral [..]; Food Supplements, Alternative Medicine; longest PFS, shortest treatment – could also be left as open question) |
Willing to accept the most appropriate treatment for her despite possible toxicities. |
History: No symptoms of the disease (ECOG PS 0), anxious because of the disease progression.
Physical examination: No signs of recurrence locally, NAD in general.
Investigations:
- Blood tests: elevated CA15-3: 275 kU/l, otherwise NAD,
- CT scans (thorax, abdomen) and bone scintigraphy: two bone metastases (left ala of ilium and 5th thoracic vertebra),
- ECG: NAD
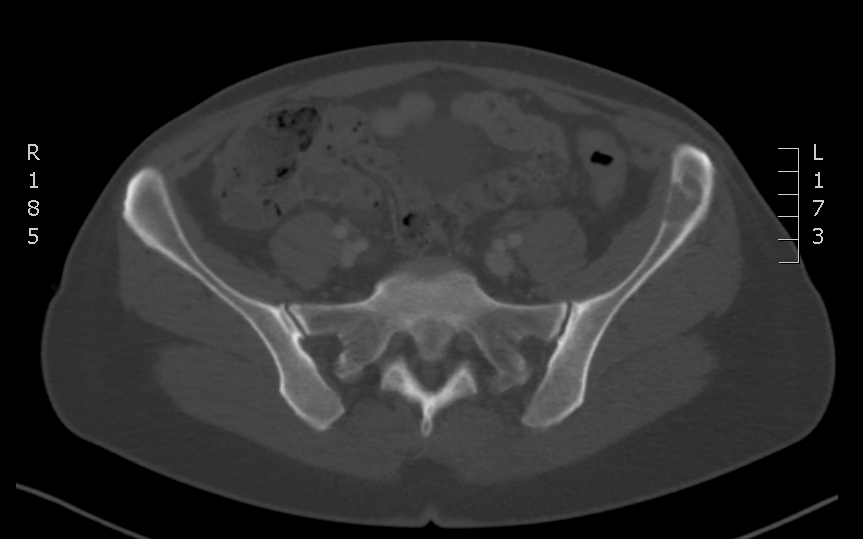
DIAGNOSIS: oligometastatic hormone positive, HER2 negative breast cancer
NAD – no abnormalities detected
1st line treatment: letrozole 2.5 mg/day and ribociclib 600 mg/day 3 weeks on 1 week off
Treatment goal: to prolong survival and maintain quality of life.
Follow-up plan according to the protocol of CompLEEment-1 study:
- 1st, 2nd month: every 2 weeks,
- from 3rd to 6th month: every month,
- from 7th to 12th month: every 2 months,
- then every 3 months.
Until 4/2019 no clinical significant adverse events were detected:
- the patient remained in good condition, fully active,
- in blood results only neutropenia grade 1 appeared, tumor marker dropped to normal:

- follow-up CT scans: stable disease
15/4/2019: admission to the hospital due to high fever with chills, pain and redness of left arm with progression of lymphedema and pain in the right shoulder with impaired mobility:
- few days before she injured finger of the left arm during gardening, later on redness of the arm appeared.
- The day before the admission she consulted her family doctor because of the fever who prescribed penicillin tbls
Physical examination:
- erysipelas of left arm with intensive lymphedema,
- impaired mobility of right arm,
- cardiocirculatory stable.
Investigations:
- blood results: leucocytes 4.05x 109, neutrophils 3.56x 109, C reactive protein 348 mg/l, procalcitonin 71.9 μg/l, liver and kidney tests normal,
- microbiologic samples: remained sterile,
- MRI of cervical and upper thoracic spine: no metastases but herniated disk at C4/5 and C5/6 level with compression of right 5th cervical and bilateral 6th cervical spinal nerve – referral to orthopaedist advised
ribociclib stopped, letrozole continued + intravenous penicillin + supportive therapy
discharge home: 25/3/2019 with peroral antibiotics, follow-up CT scans ordered.
9/5/2019 – first follow-up after the discharge:
- in good condition, lymphedema of left arm less prominent,
- blood tests: NAD,
- CT scans: stable disease,
- ribociclib introduced again at the full dose 600 mg/day.
Due to recurrent neutropenia grade 3 the dose was reduced to 400 mg/day in 9/2019.
NAD till follow-up visit in 10/2021:
- clinical stable,
- blood results: elevated CA 15-3,
- CT scans: progressive disease of the right pleura with pleural effusion and enlarged mediastinal lymph nodes.
Duration of first line treatment: 464 months
Genetic tests:
- no germline mutations,
- PIK3CA mutation in primary tumor absent,
- Wild type dihydropyrimidine dehydrogenase gene → normal metabolism of fluorouracil assumed.
NAD – no abnormalities detected
1.10/2021 – 9/2022: capecitabine 2000 mg bid 2 weeks on 1 week off: stable disease until progression in lungs: 11 months
- the dose was reduced to 800 mg bid due to hand-food syndrome (despite the fact that she was supposed to have a good metabolism of fluorouracil according to genomic testing)

2. 10/2022 till present: fulvestrant 500 mg i.m. monthly and everolimus 10 mg/day: partial regression in lungs 4 months
- so far without significant adverse events, prefers this treatment to capecitabine
1. The patient was treated for metastatic hormone positive, HER2 negative breast cancer with 1st line ribociclib and letrozole:
- She remained progression free for almost 4 years.
- She suffered one serious adverse event: erysipelas with sepsis due to delayed consultation of the doctor after the injury to her finger during gardening.
2. She is now on her 3rd line of treatment, fully active with good quality of life.
TAKE HOME MESSAGE:
- Education of patients about risk of infection during treatment with ribociclib is important for minimising adverse events.
- Patients frequently forget our verbal instructions or do not read carefully the visit reports.
- Patients‘ handouts with the most important facts about the therapy they are receiving might improve their compliance with our instructions.