IMMINENT LIVER FAILURE DURING TREATMENT WITH RIBOCICLIB AND LETROZOLE IN PATIENT WITH METASTATIC BREAST CANCER
59 years old female presented with primary metastatic breast cancer (bone metastases) in 2018:
- Tumour biology: ER 100%, PR 30%, HER2 negative, Grade II, MIB-1 1 %, PIK3CA mutation found in primary tumour,
- genetic testing negative,
First line treatment with ribociclib and letrozole:
- Drug induced liver injury appeared at the beginning of 4th cycle due to which the drugs were discontinued. After 3 months liver function normalised.
- The patient remained progression free for 3 years with anastrozole monotherapy till 1/2022 and with no consequences regarding liver toxicity.
From then on the disease is progressing more quickly – she is now receiving 4th line of therapy with capecitabine.
Female, born 1959
The patient presented with palpable left breast carcinoma in 2018. Chest X ray and ultrasound of abdomen showed no distal metastases.
Otherwise she was in good condition without chronic medications and significant past medical events.
Left modified radical mastectomy was done:
- invasive ductal carinoma, 7 cm large,
- 10/29 lymph nodes positive,
- ER 100%, PR 30%, MIB-1 1%, grade II, HER2 negative,
- CT scans (thorax, abdomen) and bone scintigraphy ordered
|
Clinical information |
|
|
Age |
59 years |
|
Menopausal status |
pomenopausal |
|
Visceral disease |
No |
|
Adjuvant endocrine treatment duration (Subcategories: prior/on/after adjuvant) |
No |
|
Metastasis localization and numbers |
Bones, multiple ( approx. 10 according to scintigraphy) |
|
Medication |
None |
|
Geriatric assessment (if available) |
/ |
|
Comorbidities and concomitant treatment |
None |
|
Previous treatments |
/ |
|
Genetic test results (if available) |
negative |
|
Personal information |
|
|
Lifestyle (Subcategories: Activities, hobbies, habits, smoking, eating habits, obesity, exercise) |
Current smoker (few cigaretes per day for 30 years), regular exercise |
|
Patient treatment preferences (Subcategories: Cancer treatment: IV, Oral [..]; Food Supplements, Alternative Medicine; longest PFS, shortest treatment – could also be left as open question) |
Willing to accept the treatment suggested by the oncologist |
History:
- Family history positive for breast cancer (one aunt had breast cancer before the age of 30, grandfather had lung cancer, both two were mother‘s relatives).
- Without symptoms of disease but lost of weight for 2 kg (related to the stress due to the diagnosis of cancer).
- No pain or use of analgesics.
Physical examination:
- ECOG PS 0,
- operative scar with no signs of infection, right breast without palpable lumps,
- physical examination: NAD
Blood tests:
- Within the normal range including tumor marker CA15-3
DIAGNOSIS:
primary metastatic hormone positive, HER2 negative breast cancer with bone metastates
NAD – no abnormalities detected
Treatment goal: to prolong survival and maintain good quality of life.
8/2018: 1st line therapy with letrozol 2.5 mg/day and ribociclib 600 mg/day 3 weeks on, 1 week off were introduced until progressive disease or unacceptable toxicity.
ECG before the beginning of the treatment: within the normal range including the lenght of QT interval
Patient monitoring strategy:
First two months follow up visit every two weeks, then monthly up to 6 months
Follow up at the start of 1b, 2a, 2b and 3rd cycle (10/10/2018) within normal limits
Follow up visit at the beginning of 4th cycle (7/11/2018):
- History and physical examination NAD,
- blood results: hepatopathy grade 4 – ribociclib but not letrozole discontinued,
- consultation with gastroenterologist: viral hepatitis tests and tests for autoimmune hepatitis ordered (both negative), follow up visit after 1 week
Subsequent liver tests:
Units:
- AST, ALT, gamma GT, alkaine phosphatase: μkat/l
- bilirubin:μ mol/l
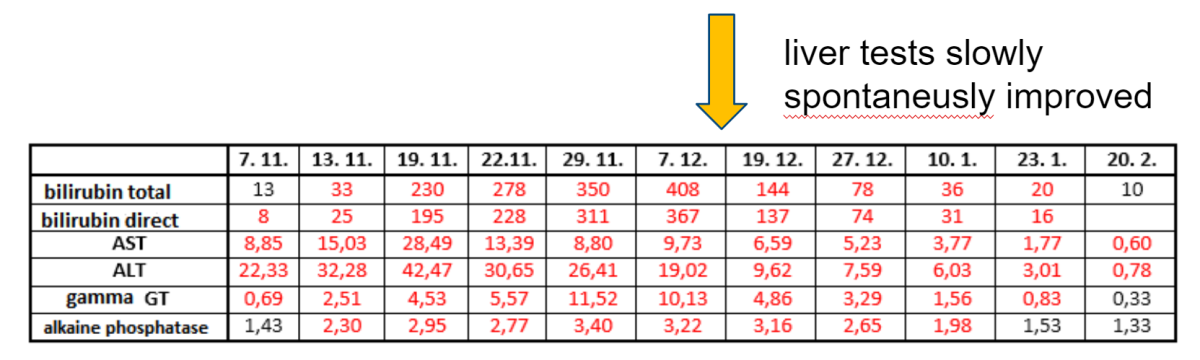
13/11: discontinuation of all drugs
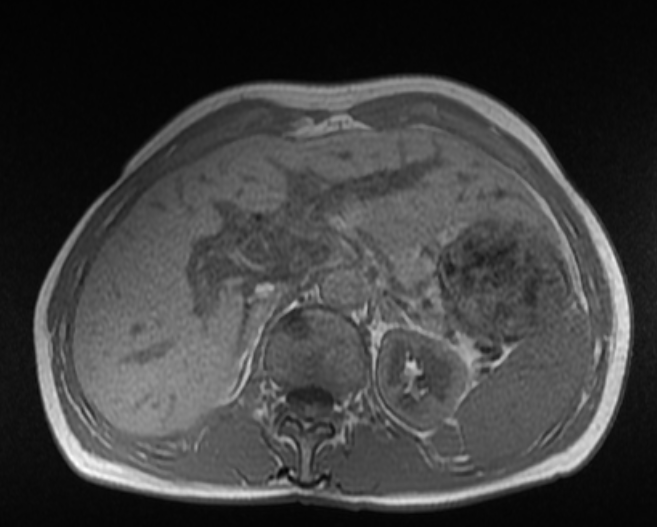
19/11: the patient became symptomatic: jaundice, fatigue, loss of appetite and weight:
- MRI of liver: parenchymal liver damage with signs of sinusoidal obstruction syndrome,
- metylprednisolone 1 mg/kg for 7 days introduced without significant improvement of liver tests
- Liver biopsy was not indicated as the result will not influence treatment decision,
- synthesis liver function was only moderately impaired (slightly pathologic INR and albumin levels)
- Supportive care: caloric supplements, osmotic laxatives to achieve loose stools
1/2019: symptoms improved to normal
- CA15-3 negative
- bone scintigraphy: stable disease
30/1/2019: introduction of anastrozole 1 mg/day
- Liver tests remained normal,
- 2/2019: zoledronic acid 4 mg i.v. every three months due to bone metastases was introduced
10/2019 the patient without symptoms, CT scans (thorax, abdomen): stable disease
Genetic tests:
- no germline mutations,
- PIK3CA mutation found in primary tumor
- Wild type dihydropyrimidine dehydrogenase gene → normal metabolism of fluorouracil
1. 1/2019 – 12/2021 anastrozole: stable disease until progression in bones - 3 years
2. 1/2022 – 4/2022 fulvestrant 500 mg i.m. monthly and alpelisib 300 mg/day: progressive disease in bones - 4 months
3. 5/2022 – 9/2022 exemestane 25 mg/day and everolimus 10 mg/day: - 5 months
- The dose of everolimus reduced to 5 mg/day due to transient hepatopathy grade 2
- progessive disease in bones
4. 10/2022 till present: capecitabine: stable disease - 4 months
- The patient suffered from grade 4 hepatopathy due to ribociclib which was luckily reversible and left no consequences.
- Different CDK4/6 inhibitor was not introduced due to severity of the hepatopathy.
- The disease had indolent course initially but did not respond to two lines of further endocrine therapy → NGS sequencing of metastasis was not done due to bone only disease and other treatment options left.
- 4th line of therapy – capecitabine looks promising considering that tumor marker is finally decreasing.
TAKE HOME MESSAGE:
- frequent monitoring of patients on ribociclib is urgent
- for safe and effective patient treatment:
- importance of patient‘s compliance with our follow up instructions